

Definition of the disease. Causes of the disease
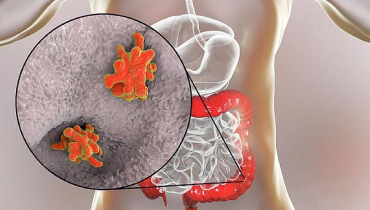
Amoebiasis (Amoebic Dysentery) is an acute and chronic disease caused by pathogenic strains of Amoebic dysentery. Penetrating into the body, they lead to intestinal ulceration accompanied by moderate intoxication, stool disorders, weight loss and sometimes abscesses in the liver, intestines, lungs and brain. The disease can be long-lasting, sometimes leading to death, especially in weakened patients and in the absence of medical care.

The pathogen
The Russian scientist F. A. Loesch was the first to describe the pathogen and prove its pathogenicity in 1875. Now at least 22 strains have been isolated, 9 of which are pathogenic, and the remaining 13 are most likely not pathogenic to humans.
Changing in the course of their lives, amoebae go through two stages of development:
- a vegetative, or active, stage in the form of a trophozoite;
- a resting or “dormant” stage in the form of a cyst.
The vegetative stage subdivides amoebae by function and structure into large vegetative, lumen, and tissue. All of them, suddenly entering the external environment, die within 30 minutes.
Large vegetative trophozoites (forma magna) reach 20-60 µm. This form of amoebae moves by translational thrusts. It contains a nucleus and cytoplasm, the main part of the cell. The cytoplasm is divided into a vitreous transparent mass and an inner liquid layer with digestive vacuoles in which amoebae digest captured erythrocytes. In acute amoebiasis, large trophozoites are detected in fresh feces – “warm feces”.
Able to break down protein molecules. Have surface pectins, which amoebae use to attach to the intestinal mucosa.
Lumenal vegetative trophozoites (forma minuta) are much smaller than large forms: they reach 15-20 µm. Such trophozoites are sedentary. They have a single nucleus, which is not visible without staining. Their cytoplasm contains small vacuoles, but already without erythrophytes. Luminal trophozoites live in the upper part of the colon, feed on bacteria, multiply, and do not cause obvious harm. They are detected in the feces in acute amoebiasis at the beginning of recovery, in chronic amoebiasis, as well as in carriers of amoebiasis, but to detect them, deep bowel lavage or examination of the final portions of the stool after taking salt laxatives must be performed. In the lower colon, when conditions gradually deteriorate, such as lack of fluids, disruption of bacterial flora, ingestion of medications, or changes in pH, they usually change to cystic form, which gradually escape into the environment. If the body’s defenses are weakened, the lumen trophozoites may change into a larger vegetative form and become aggressive.
Tissue vegetative trophozoites are formed from the luminal form, but look similar to the vegetative form. They reach 20-25 µm, are motile, and parasitize by penetrating into the mucosa of the large intestine and affecting the intestine. They are detected only in acute amoebiasis in the affected organs; they are very rarely found in liquid feces – in the decay of intestinal ulcers.
Cysts are formed from the lumen in the lower parts of the large intestine. They have a rounded shape and reach 8-15 microns in size. They are immobile, covered with a dense shell of chitin and contain chromatoid bodies (RNA and protein) and glycogen. Depending on the maturity of cysts, they contain from 1 to 4 nuclei. More often they are detected in patients with chronic amoebiasis and parasitic carriers. They are very resistant in the external environment, preserving in feces at room temperature for 2 weeks or longer, in freezing to -21° C – for no more than 3 months, in water – up to 8 months. When heated to 100°C and boiled, they quickly die. Standard household disinfectants with chlorine have practically no effect on cysts. Soap and cresol preparations, bicarbonate solution 1:1000, and 3% solution of carbolic acid can have an effect on them.
Epidemiology
Amoebiasis is a widespread disease, mainly found in Southern and Western Africa, Central and South America, as well as in India, China and Korea. In Russia, mainly single cases are registered, mainly in the southern regions, the Caucasus and the Far East. Though lately the rate of the disease has been increasing in our country. Perhaps, it is connected with inflow of migrants from border regions and tourism development.
On the average there are 50 mln. cases of amoebiasis registered in the world annually, of which about 100 thousand end up in death. This disease ranks third among parasitic diseases by the number of deaths. Intestinal amoebiasis accounts for about 90% of cases, while the remaining forms are extraintestinal.
The source of infection is a person (patient or carrier). Amoebae in cyst form enter the environment with their feces.
Mechanism of transmission is fecal-oral. It includes water, food, contact and sexual (oral-anal) routes of transmission. Infection can occur by ingestion of any substance (water, food, dirt, fingers) that has come into contact with or contains some part of the feces of an infected person. Mechanical vector vectors can be cockroaches and flies. In extremely rare cases, homosexuals and patients with secondary immunodeficiency may be infected when amoebiasis enters the wound directly.
A person with amoebiasis risks transmitting the infection to family members, but the risk is low, especially if the person follows personal hygiene rules: carefully washing their hands after the bathroom and before cooking.
Situations that increase the risk of infection
- Visiting tropical countries with low sanitation;
- interacting with immigrants from tropical countries with poor sanitation;
- Disregard for personal hygiene practices;
- Consuming raw, uncontaminated water from open sources and water systems;
- Homosexual contact;
- Presence of mental disorders.
Immunity after the disease is fragile and weak, and reinfection is possible. Even a large number of antibodies produced, e.g. in amoebic liver abscesses, do not save against the progression of amoebiasis.
Symptoms of amebiasis
The incubation period – the time when the first symptoms appear after infection – lasts from 7 days to 3-6 weeks or several months. Most cases of infection are either asymptomatic (carriage) or asymptomatic with a mild intestinal form or subclinical (detected by tests, no symptoms). Such a condition can last for many years, but there is always a risk of transition of the disease into an overt form.
Acute intestinal amoebiasis (colitis or dysentery)
The disease begins gradually, with moderately pronounced abdominal pain. They are usually localized in the right and left iliac area. Sometimes they acquire a cramp-like character. It is accompanied by mild diarrhea. The amount of feces is usually small and tends to decrease. Due to ulcerative defects in the intestinal mucosa, there are impurities (streaks) of blood in the feces. The more pronounced the process, the more impurities, up to a characteristic crimson color of the feces. There is a slight intoxication: weakness, malaise, fever.
In the non-serious acute course, despite clearly pronounced diarrhea, the well-being remains relatively satisfactory. Young children may quickly develop dehydration and intoxication, skin firmness and elasticity decrease, the child becomes thin, and convulsions occur. The process usually lasts for 3-6 weeks.
Chronic intestinal amoebiasis
If the process then subsides, leaving only mild abdominal discomfort and unstable stools for a week or a couple of months, there may be a cure. But more often, after a period of relative calm, the symptoms return. And so it goes on for decades: periodic bloating and pain in the abdomen, including pressure, unstable stool with periods of diarrhea, constipation and blood admixture, the liver gradually increases in size, weakness, nausea, loss of appetite, increasing emaciation. Outwardly, the asthenicism and pallor of the patients draws attention. Without treatment, this form of the disease will sooner or later lead to complications and premature death.
Extraintestinal amoebiasis
There are five forms of extraintestinal amoebiasis:
- Amoebic liver abscess;
- pleuropulmonary amoebiasis;
- Amoebic pericarditis;
- Cerebral amoebiasis;
- Skin amoebiasis.
Amoebic liver abscess is the most common form of extraintestinal lesion. It can occur both after previously diagnosed or current intestinal amoebiasis (up to 40%) or be the first manifestation of the disease. It occurs more often in adult men, especially those with alcohol addiction.
As a rule, the right lobe of the liver is affected because of the peculiarities of the blood supply. The size of the abscess can reach up to 20 cm. Suddenly a fever of irregular (septic) type appears: the body temperature rises rapidly to 40°C and within a day falls sharply, sometimes to normal, then rises again. The difference in these fluctuations per day is more than 2°C. Children may simply have a subfebrile fever of 37.1-38.0°C. The rise in temperature is accompanied by severe chills and sweating (more often at night). There is also severe pain in the right subcostal area, which is irradiated to the right shoulder and shoulder blade. In 20% of cases, there may be no pain, and the cause of the disease may remain unclear for a long time.
Among other things, the liver increases in size, palpation of the right subcostal area is painful, and jaundice may develop, which is an unfavorable sign indicating that the liver is malfunctioning.
Pleuropulmonary amoebiasis can occur in two cases: when amoebas spread from the intestine through the blood or, more often, when a liver abscess bursts through a fistula into the diaphragm and lungs. This results in lung abscesses and specific pleural empyema – accumulation of pathological fluid in the pleural cavity, sometimes pus. There are pains in the chest, dyspnea, the body temperature rises, the patient feels chills, there are signs of severe intoxication: severe weakness, sweating, dizziness, nausea. Often, hemoptysis joins, sometimes with pus due to exposure to bacteria.
Amebic pericarditis develops when a hepatic abscess ruptures from the left lobe into the pericardium, the pericardial pouch. Cardiac tamponade develops, and severe dizziness, weakness, and fainting occur – often fatal.
Cerebral amoebiasis occurs when amoebas enter the brain through the blood. It develops very rapidly. It is characterized by the most severe course with almost inevitable death.
Amoebiasis of the skin develops in patients with a weakened immune system. Ulcerative elements appear in the area of the fistula, more often in the perianal area, in the liver area and in the genital area (if amoebas from feces get on the damaged skin surface). The lesions look like erosions or painful ulcers of various shapes and sizes with raised and undermined edges. The bottoms of the defects are often red-brownish, sometimes with a brownish tinge, the smell is foul-smelling.
Amoebiasis in pregnant women
Amoebiasis is more severe in pregnant women and in the early postpartum period, especially after administration of immunosuppressive glucocorticosteroids, than in nonpregnant women. It is possible to develop fulminant amoebic colitis. It is a suddenly occurring condition with severe intoxication, severe abdominal pain, which is caused by total ulcerous lesions of the intestinal mucosa. It is accompanied by intestinal bleeding, intestinal perforation and peritonitis. The risk of mortality is up to 70%. No specific effect on the fetus has been observed.

Pathogenesis of amebiasis
The entrance gate is the oral cavity. Dysentery amoeba cysts enter the body through it. They pass through the stomach into the small intestine unchanged. There, the cysts lose their protective shell, resulting first in the formation of a 4-nuclear trophozoite – a parasite in the active feeding stage, and after a simple division – 8 mononuclear amoebae, which continue to descend lower, reaching the upper sections of the large intestine – the cecum and colon.
In the intestine, the amoebae further develop into their lumen form, reproduce and feed. They absorb bacteria and detritus – product of tissue decay. At this stage the amoeba is a saprophyte and does not cause inconvenience to the body.
This can go on indefinitely, but sooner or later there comes a trigger: reduced immunity, penetration of other parasites, development of intestinal infection, stress, malnutrition, etc. After the trigger, the amoebae modify into tissue forms and produce destructive enzymes that damage the mucous membrane of the large intestine.
By invading the intestinal wall, the amoebae begin to multiply actively, causing even more damage and suppuration – a micro-abscess. Over time, the abscess opens into the intestinal lumen, and an ulcer forms on the intestinal wall. The defects look like craters with uneven raised edges. Inflammatory reaction around the ulcer is weakly expressed, the bottom of the defect consists of dark brown dead tissue. In terms of maturity, the ulcers can be primary, in advanced stage or scarring. They are solitary or coalesce into extensive erosions.
In severe cases, the involvement of the colon can become total, but more often only the blind and ascending part of the intestine is affected. With a long course of the disease in the intestinal wall due to the constant confrontation of the destructive process and regeneration can form a lot of connective granulation tissue. This contributes to the thickening of the wall and narrowing of the intestinal lumen, i.e. intestinal stricture. Parasites localize mainly on the border of healthy and dead tissue, actively absorbing erythrocytes.
As the process progresses, the amoebae penetrate into the mesenteric vessels and spread through the blood to various organs with a rich blood supply. As a result, liver abscesses appear (in 95% of cases), brain and lungs. This process can be considered as metastasis. At first the abscesses are small necroses, but then they coalesce to form large lesion areas.
A liver abscess has three conditional zones: an area of central necrosis, lesions of the stroma (organ skeleton) and an outer fibrin zone containing amoeba trophozoites. The necrosis zone contains detritus, erythrocytes and other substances, except bacteria. The color of the contents is yellow-brown to brown. If a fistula (pathological opening) occurs in the intestine or liver, there is an amoebic lesion in the skin and sometimes in the perianal area.
Amoebae do not die during parasitization because they can avoid the aggressive effects of the immune system. They disrupt the production and promote the breakdown of immunoglobulin A, which plays an important role in protecting mucous membranes and skin, thus suppressing T-cell immunity.
When encountering neutrophils, a type of white blood cell, amoebae can engulf and destroy these immune cells. This will result in the release of enzymes and free radicals that will increase tissue damage.
In general, the immune system can only partially and temporarily limit the affected area, but it cannot resist and defeat the disease on its own.
Classification and stages of amebiasis
The International Classification of Diseases (ICD-10) distinguishes 10 forms of the disease:
- A06.0 Acute amoebic dysentery (acute intestinal involvement).
- A06.1 Chronic intestinal amoebiasis (chronic bowel disease)
- A06.2 Amoebic nondysenteric colitis (ulcerative involvement of the large intestine)
- A06.3 Amoeboma of the bowel (tumor-like bowel lesion)
- A06.4 Amoebic liver abscess (can be either a complication of the intestinal process or an independent form of the disease)
- A06.5 Amoebic pulmonary abscess (lung involvement, sometimes with liver).
- A06.6 Amoebic brain abscess (brain involvement, sometimes with liver and lungs).
- A06.7 Cutaneous amoebiasis (ulcerative skin lesion).
- A06.8 Amoebiasis infection of other localization (appendix or penile head).
- A06.9 Amoebiasis unspecified.
The World Health Organization (WHO) classifies forms of amoebiasis into two groups:
- The asymptomatic form.
- Manifest form
Iintestinal amoebiasis – includes amoebic dysentery and nondysenteric amoebic colitis.
Extraintestinal amoebiasis – includes hepatic amoebiasis (acute form and liver abscess), pulmonary amoebiasis and other extraintestinal lesions.
According to the type of the disease there are three forms:
- The typical form – the development of intestinal amoebiasis, amoebic dysentery or acute amoebic colitis;
- Atypical form – latent, asymptomatic course of amoebiasis;
- Lightning form – sudden development of the disease with signs of severe intoxication, severe abdominal pain caused by total lesion of the intestinal mucosa, intestinal bleeding, intestinal perforation, peritonitis and high mortality rate.
According to the severity of intestinal amoebiasis there are three grades:
- mild – slow onset without signs of intoxication or its minimal manifestations, temperature is normal or does not exceed 38.0°C, no abdominal pain, stool of normal consistency or mushy up to 3 times a day, no blood in the stool, one segment of the intestine is affected more often, changes in clinical blood tests are observed, no complications;
- moderate – subacute onset, within a week, moderately marked intoxication and febrile temperature (38-39°C), abdominal pain of moderate intensity, characterized by mushy or liquid stools with blood admixture up to 10 times a day moderately pronounced signs of inflammation in the coprogram, increased levels of eosinophils in the blood and erythrocyte sedimentation rate, ulcerative and necrotic lesion of several segments of the large intestine, sometimes complications develop;
- severe – the disease begins acutely, severe intoxication and febrile fever persist for more than a week, intense intense abdominal pain is observed, tenesmus may occur – sharp cramping pain in the rectum, stool becomes liquid with blood and mucus, frequency of defecation – 10 times a day, pronounced changes in clinical blood count and co-program, several intestinal segments are affected, up to total, complications develop.
According to the presence of complications, the disease can proceed:
- without complications;
- with intestinal and extraintestinal complications.
Complications of amebiasis
Intestinal complications:
- ulcer perforation, more often in the cecum, with the development of intestinal bleeding, peritonitis, and abscess formation in the abdominal cavity;
- amoebic appendicitis;
- amoeboma – tumor-infiltrate formation in the intestinal wall, consisting of collagen, fibroblasts and cellular elements;
- intestinal stricture – adhesions process, can manifest as constipation and bowel obstruction;
- anemia and emaciation – develops with a prolonged chronic course of the disease.
Extraintestinal complications:
- amoebic pericarditis – develops from an abscess bursting through the diaphragm into the pericardium, can cause cardiac tamponade and lead to death;
- pleural empyema – occurs because the abscess has burst through the blood or diaphragm into the lungs, and is manifested by chest pain, cough, shortness of breath, sputum with blood and pus, tremendous chills and fever; blood levels of leukocytes, neutrophils and eosinophils are increased
- fulminant amoebiasis – occurs more often in weakened children and pregnant women, characterized by an abrupt onset with hectic fever, total intestinal damage, severe toxemia, intestinal bleeding and unfavorable prognosis;
- skin amoebiasis – develops in weakened patients, more often in the perianal area;
- cerebral amoebiasis – characterized by acute onset with severe cerebral symptoms, the prognosis is unfavorable.
Intestinal complications develop more often. Risk factors include: immunodeficiency state, early childhood and pregnancy.
Diagnosis of amoebiasis
Diagnosis is based on the history – being in an area dangerous for amoebiasis – and laboratory examination data, including specific tests to detect the pathogen.
Intestinal amoebiasis is accompanied by intestinal pain and stool disorders. It must be distinguished from:
- acute and chronic intestinal infections – shigellosis, salmonellosis, escherichiosis, campylobacteriosis, etc;
- other parasitic diseases – giardiasis, balanceidiasis, intestinal schistosomiasis, etc;
- intestinal inflammation of non-infectious nature – nonspecific ulcerative colitis and Crohn’s disease;
- Pseudomembranous colitis – the development of this disease is associated with long-term administration of antibiotics;
- diverticulitis;
- ischemic colitis;
- intestinal tumor (with amoeboma).
Extraintestinal amoebiasis must be distinguished from:
- purulent abscesses of the liver, brain, and kidneys;
- echinococcal cysts;
- hepatocellular carcinoma, a malignant tumor of the liver.
Laboratory and instrumental diagnosis of amoebiasis involves:
- Clinical blood count. In intestinal amoebiasis there is a moderate increase in eosinophils and basophils. In extraintestinal amoebiasis there is a moderate increase in leukocyte levels with a shift to the left to young neutrophil forms, increased erythrocyte sedimentation rate (ESR), concentration of eosinophils and basophils.
- Biochemical blood analysis. In extraintestinal amoebiasis, increased alkaline phosphatase, total bilirubin, AST and GGT may be noted.
- Coprogram. In the feces, leukocytes, erythrocytes, mucus, and various forms of amoebae are found.
- Serologic specific tests: immunofluorescence reaction (RIF) or enzyme immunoassay (ELISA). Mainly used to diagnose extraintestinal amoebiasis when the pathogen cannot be detected in feces.
- Fecal PCR is a polymerase chain reaction. This is a promising method of investigation, but it does not give information about the disease or the carrier. It can only be used to detect amoebas in the intestine.
- Colonoscopy is a microscopic examination of feces. In this case, this method is used to search for large vegetative forms of amoebae only in freshly collected liquid stools, as they lose mobility and die after 15-25 minutes. A salt laxative can be used to make the examination more reliable. You can increase the storage time of the stool by using a jar of preservative. Enrichment methods such as ether-formalin precipitation are desirable. Examination of the formalized stool may reveal luminal forms of amoebae, and if cysts are detected, stools with longer storage time will be suitable, but the diagnosis will be questionable. In acute amoebiasis, only large vegetative amoebae are more often isolated in the feces, and in the convalescence period, lumen amoebae and cysts. The morphological similarity of dysentery amoeba and nonpathogenic amoeba species, such as Entamoeba dispar, causes a big problem. It is practically impossible to distinguish them in ordinary microscopy, especially for an untrained laboratory technician. Therefore, it is advisable to take the tests in specialized laboratories.
- Microscopy of material obtained by abscess puncture. Allows detection of amoebae. In extraintestinal amoebiasis, the material should preferably be taken from the border of healthy and diseased tissues or the inner surface of the abscess capsule.
- Recto- and colonoscopy – visualization of lesions of the large intestine. It allows detection of intestinal ulcers, amoebomas and the amoebas themselves – those that digest red blood cells. As a rule, a focal lesion is detected.
- Ultrasound or CT scan of abdominal and thoracic organs. It is indicated if extraintestinal amoebiasis is suspected. They reveal localization, size and number of abscesses, allow to monitor the result of treatment.
Treatment of amoebiasis
Treatment of patients with amoebiasis is possible both in an inpatient and outpatient setting. The choice of place of treatment depends on the severity of the condition and localization of the process.
Patients with moderate and severe course, extraintestinal form of the disease, complications, as well as for epidemiological indications should be hospitalized.
Diet is indicated for all patients. It involves mechanical and chemical sparing of the intestine. For this purpose, it is necessary to exclude alcohol, fatty, fried, spicy, smoked foods and sodas. Sufficient volume of fluids is necessary.
Etiotropic therapy, aimed at the destruction of the pathogen, is used in all forms of the disease and carriage. In extraintestinal amoebiasis drugs of 5-nitro-imidazole group, dehydroemethine dihydrochloride, chloroquine, paramomycin, etc. are used. In intestinal amoebiasis, drugs that work only in the intestinal lumen, such as Etofamide, and 5-nitro-imidazoles are used.
In large liver abscesses (more than 6 cm) surgical manipulations are performed to reduce and eliminate the focus – drainage of the abscess percutaneously or with vacuum suctioning. In rare cases surgical intervention is indicated.
With accession of secondary bacterial flora the treatment is connected to antibacterial agents. At the same time as the treatment and in the recovery period appoint replacement and recovery drugs, which normalize the intestinal microflora – probiotics and saccharomycetes. So far, these drugs do not have a sufficient evidence base.
Criteria for recovery:
- persistent normalization of body temperature and stool quality within 3 days;
- disappearance of marked intoxication;
- normalization of general laboratory blood parameters;
- absence of pronounced inflammatory process in the intestine according to coprogram;
- disappearance of intestinal ulcers according to colonoscopy;
- tendency to normalization of the liver and reduction of its size.
Rehabilitation for amoebiasis of mild course, carriage and most uncomplicated forms of acute amoebiasis of moderate course, as a rule, is not required – a short diet and probiotic drugs are enough.
In severe, chronic and complicated forms a long period of compliance with dietary recommendations, improving the regeneration of intestinal mucosa, replenishment of protein-energy deficiency and restoration of microbiocenosis under control of specialists – infectious disease specialist, gastroenterologist and nutritionist. If irreversible organic pathology develops, the help of a surgeon may be required.
Prognosis. Prevention
If timely medical care is given to a patient with uncomplicated intestinal amoebiasis, the prognosis is usually favorable. In the presence of risk factors, the development of extraintestinal amoebiasis and complications, the prognosis is serious, up to and including death. The probability of death depends on the location of the lesion and initial health indicators.
No specific prophylaxis has been developed. Prophylactic use of chemotherapeutic agents is not recommended.
Non-specific preventive measures:
- Monitor the condition of the water supply, keep sewage and human feces out of it, and disinfect the water.
- Drink only that water and eat only that food in which you are sure of its quality. Do not drink uncontaminated water from rivers, lakes, fountains, from the tap, use ice from raw water, eat unwashed fruits and vegetables, unpasteurized dairy products and food from the street, especially in countries with unfavorable sanitary situation. Water should preferably be boiled.
- Timely detection and treatment of patients and carriers of amoebas, disinfect their place of residence: feces and dirty laundry decontaminate with 3% lysol solution.
- Perform the act of defecation only in specially designated places, wash your hands after the restroom, before eating and cooking.









I received the package a few days ago. Thank you so very much! Everything was perfect. I do appreciate your great service and will most definitely order again from you. I'm glad to say that I can recommend you with total confidence. Thanks
Yeah! The package arrived very quickly. Thanks!
Everything is fine! Thanks!